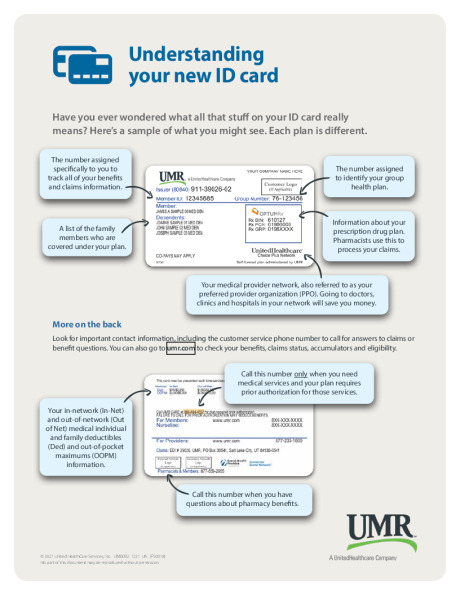
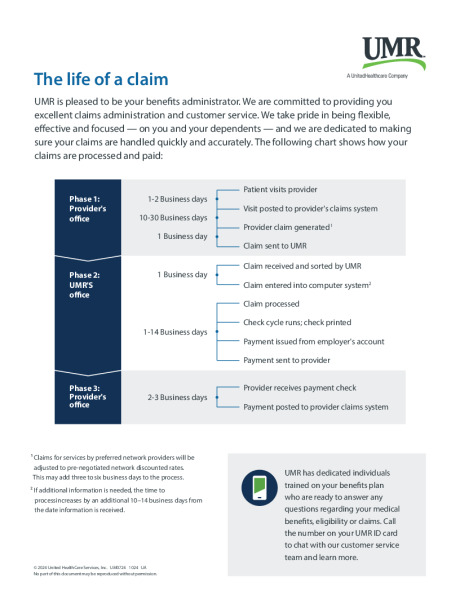
Which Medical Plan is Right? Evaluate Your Needs. Consider your prior health care usage and select plans and options that fit your lifestyle and needs. Do you take regular prescription medications? Are you anticipating surgery or non-preventive dental care? Did you experience a qualifying life event this year? Review your current plans to ensure you have the coverage you need. Review this benefits website to learn about your plan options. A little bit of planning will help you select the best plans, coverage levels, and financial programs for your unique situation. Preventive Care Covered at 100% on all medical plan options.The following services are covered at 100% by UMR prior to your preventive care visit: Routine preventive for Children*Appropriate screenings based on gender and age Newborn visits Tuberculosis testing Anemia testing Lead exposure Pelvic exam and pap test Development and behavior Lipid profile Depression Obesity and counseling Nutrition counseling*Birth to age 18 Routine preventive for AdultsAppropriate screenings based on gender and age Lipid profile Diabetes Pelvic exam and pap testing Breast exam and mammogram Bone density testing Colonoscopy Aortic aneurysm Medical Plan Comparison The charts below are a brief outline of what is offered. Please refer to the summary plan description for complete plan details. Administered by UMR, a United Healthcare Company UMRValue HSA Plan UMRBase HSA Plan **New** UMR Value PPO Plan UMRPremium PPO Plan Annual Deductible Individual $5,000 $2,500 $5,000 $2,000 Family $10,000 $5,000 $10,000 $4,000 Coinsurance You pay 30% You pay 20% You pay 30% You pay 10% Maximum Out-of-Pocket Individual $6,900 $6,900 $6,900 $6,600 Family $13,800 $13,800 $13,800 $13,200 Physician Office Visit Primary Care 30% after deductible 20% after deductible $50 copay $30 copay Specialty Care 30% after deductible 20% after deductible $100 copay $45 copay Preventive Care Adult Periodic Exams Covered 100% Covered 100% Covered 100% Covered 100% Well-Child Care Covered 100% Covered 100% Covered 100% Covered 100% Diagnostic Services X-ray and Lab Tests 30% after deductible 20% after deductible 30% after deductible 10% after deductible Complex Radiology 30% after deductible 20% after deductible 30% after deductible 10% after deductible Urgent Care Facility 30% after deductible 20% after deductible 30% after deductible $55.00 copay Emergency Room Facility Charges 30% after deductible 20% after deductible $500 copay 100% after $200.00 copay(waived if admitted) Inpatient Facility Charges 30% after deductible 20% after deductible 30% after deductible 10% after deductible Outpatient Facility and Surgical Charges 30% after deductible 20% after deductible 30% after deductible 10% after deductible Mental Health Inpatient 30% after deductible 20% after deductible 30% after deductible 10% after deductible Outpatient 30% after deductible 20% after deductible 30% after deductible 10% coinsurance deductible does not apply Substance Abuse Inpatient 30% after deductible 20% after deductible 30% after deductible 10% after deductible Outpatient 30% after deductible 20% after deductible 30% after deductible 10% coinsurance deductible does not apply UMR is here for you Understanding your EOB Find a Provider 10 ways to control healthcare costs Understanding your ID Card Understanding qualifying events UnitedHealthcare Network The life of a claim UnitedHealthcare Network High Deductible Health Plan with HSA prevQuantum Health: Your Health Advocate Telemedicinenext